Indications
1. In new lesions where it will maintain reduction during the period of ligament healing and
assure secondary reinforcement.
2. In chronic lesions where its role of “tutor” will guide the colonisation of collagen and the
reconstruction of new coracoclavicular and acromioclavicular ligaments.

Surgical Technique

Note that the patient is under general anaesthetic in a semi-reclining position releasing the shoulder.
The approach used is an anteroposteri the coracoid process at the front and the acromion at the back.
The delto-trapezial fascia is opened in “J” following the curve of the acromion by adapting itself to possible associated musculo-aponeurotic lesions.

In the event of disinsertion of the delto-pectoral yoke, the coracoid is easily approached from the front of the clavicle.
In other cases, the fibres of the anterior deltoid can be detached longitudinally perpendicular to the coracoid without requiring the disinsertion of the deltoid.
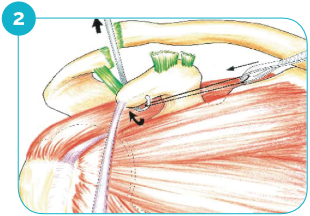
The “loop” end of the ACROLIG™ is threaded under the coracoid using the tendon guide or a dissector.
The flat part of the ligament is then threaded through the loop and pulled tight.

The first flat section of the ACROLIG™ “knots” round the clavicle from front to back, reducing the coracoidoclavicular subluxation, a stop point allowing for fixing this first time of reduction.
It is pulled back using the second flat section. It reduces both anterior and posterior subluxation while strengthening acromioclavicular ligament repair.
In old lesions: A resection of the distal cm of the clavicle is often associated with this.

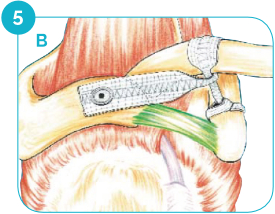
Fixation of the tensioned ligament on the acromion using the fixation staple and the locking screw perpendicular to the posterior edge of the clavicle (thickest area of the bone).
The fascia previously opened in a “J” is re-closed with staples and its suture is supported on the flat part of ACROLIG™.
Post-Operative Protocool
An immobilisation of the elbow to the body takes place for 3 weeks supporting the weight of the arm during the period of healing.
Pendular mobilisation of the arm is forbidden during this period followed by a classic protocol of re-training for one or two months.
Most sports activities (and notably contact sports) may be resumed during the post-operative 3rd month.
Product Description
The ACROLIG™ is a flat reinforcing strip of 20 X 160 mm made from Polyethylene Terephtalate, a material that is widely proven in ligament repair and reconstructive surgery.
The fiber is the result of the best manufacturing processes in compliance with current standards – ISO 13485 and CE marking – and requirements for perfect biocompatibility for implants: tests available on request. .
This ligament has been specially designed for articular triplasty, hence its unique design in three sections to suit the anatomical imperatives of the coracoid, acromion and clavicle.
FIXATION SYSTEM:
Titanium TA6V staple + locking screw specially designed for fixation through the ACROLIG™ ligament into the acromion.
OBJECTIVES FULFILLED BY ACROLIG™ (fresh and old lesions) :
- Reduction in acromioclavicular dislocation.
- Repair and strengthening of all injured ligament structures.
- Avoid the anterior subluxation effect of simple coracoclavicular cerclages.
- No need for additional pins.
- Easily tensioned using the acromial staple.
- Perfect fit of the ligament to the anatomy (no fragilisation of the clavicle by fixation through the bone or shearing by a cylindrical ligament).
- Reinforced healing of the ligament providing secondary stabilisation of the joint.
- Decrease the risk of repeated rupture.
- Early full functional recovery for work and sport.
Implants
FX290.202: ACROLIG™ Ligament
FX290.201: Fixation staple H. 10 mm
FX290.200: Locking Screw

Instruments
FX629.200: Drill guide Ø 3.2mm
FX629.201: Impactor screwdriver
FX629.202: Right grommet
FX629.203: Left grommet
FX629.204: Drill Ø 3.2mm
FX688.802: Hexagonal 2.5mm screwdriver
FX629.210: Complete instrumentation
FX629.211: Container